


Immunotherapy, which stimulates or suppresses the body’s natural immune system to fight disease, has opened exciting possibilities in cancer treatment. This type of therapy has become the fourth keystone of cancer treatment, along with surgery, radiation, and chemotherapy. A particular type of immunotherapy known as CAR-T cell therapy has proven notably effective in treating hematological cancers like leukemia.
By analyzing the CAS Content CollectionTM, the largest human-curated collection of scientific information, we can confirm the tremendous growth in both journal and patent publications relating to CAR-T cell therapy (see Figure 1). Publications have skyrocketed in recent years, demonstrating the growth in research and the commercialization of these therapies.

This research activity is starting to show results, and not just in treating hematological cancers — solid cancers are being successfully targeted by CAR-T therapies, and non-cancerous conditions like autoimmune diseases are also showing promising results with CAR-T treatments.
These therapies face persistent challenges to widespread clinical usage, and more work is needed to standardize and expand the use of CAR-T cell therapies. However, the future is bright for these breakthroughs, as the most recent study results reveal.
CAR-T cell treatment for cancer
CAR-T cell therapy uses T cells from a patient that are genetically engineered to express MHC-independent chimeric antigen receptors (CAR) to target a surface tumor antigen and kill cancer cells (see Figure 2). CARs comprise four domains: extracellular antigen binding domain, spacer or hinge region, transmembrane domain, and intracellular signaling domain.

While this approach is still considered new, it is now reaching its fifth generation (see Figure 3):
- First generation: consists of only the activation domain i.e., CD3ζ.
- Second generation: includes an additional intracellular motif — the signaling domain of costimulatory receptors such as 4-1BB/CD137 or CD28.
- Third generation: contains additional costimulatory modules, i.e., CD28, 4–1BB, ICOS, and OX40.
- Fourth generation: constructed using second-generation designs with a transgenic cytokine, usually IL-12, embedded in a nuclear factor of activated T cells (NFAT) cassette.
- Fifth generation: consists of transcription factors such as STAT3, which activates the JAK/STAT pathway eventually leading to the secretion of cytokines.

The main disadvantage of the first generation was the relatively short persistence time of CAR-T cells in patients. The development of the second generation extended their persistence and thus improved the treatment results. Currently, all FDA-approved CAR-T cell therapies are based on the second-generation type of construct. The third, fourth, and fifth generations are all designed to improve T cell proliferation and persistence, but they are still in trial phases.
CAR-T cell therapy has been effective at treating hematological malignancies such as acute lymphoblastic leukemia (ALL), chronic lymphocytic leukemia (CLL), and multiple myeloma (MM). Currently, there are six FDA-approved CAR-T cell therapies, with four targeting CD19 for treating B cell leukemia and lymphoma and two targeting B cell maturation antigen (BCMA) for treating relapsed/refractory myeloma (see Figure 4).
| CAS Registry Number | Costimulatory Domains | Brand and Generic Names | Company Name | Target Antigen/ Antibody | Targeted Cancers | Year of Approval |
|---|---|---|---|---|---|---|
|
4-1BB + CD3ζ |
KYMRIAH (Tisagenlecleucel) |
Novartis Pharmaceuticals Corporation |
CD19 |
R/R CAYA |
2017 |
|
|
CD28 + CD3ζ |
YESCARTA® |
Kite Pharma, Inc. |
CD19 |
R/R LBCL |
2017 |
|
|
CD28 + CD3ζ |
TECARTUS® |
Kite Pharma, Inc. |
CD19 |
R/R MCL |
2020 |
|
|
4-1BB+ CD3ζ |
BREYANZI® |
Juno Therapeutics, Inc. |
CD19 |
R/R LBCL |
2021 |
|
|
4-1BB+ CD3ζ |
ABECMA® |
Celgene Corporation, a Bristol-Myers Squibb Company |
BCMA |
R/R MM |
2021 |
|
|
4-1BB + CD3ζ |
CARVYKTI® |
Janssen Biotech, Inc., and Legend Biotech |
BCMA |
R/R MM |
2022 |
Figure 4: Targeted cancers: R/R, relapsed or refractory. CAYA, children and young adults. LBCL, large B-cell lymphoma. MCL, mantle cell lymphoma. MM, multiple myeloma. B-ALL, B-cell acute lymphoblastic leukemia
CAR-T cell therapy in solid tumors and cancers
CAR-T cell therapy’s success in treating blood cancers is an outstanding breakthrough, and researchers are aiming to apply this method to solid cancers too. Current cumulative evidence shows that this could be a viable therapeutic strategy.
Clinical trials for pancreatic, colorectal, and hepatocellular carcinomas demonstrated the inhibitory effect of CD133-CAR-T-cells on the metastatic potential of the cancers. In addition, other varieties of antigen targets for pancreatic cancer CAR-T cell therapy, such as CD24, MUC-1, PSCA, mesothelin, and FAP, have been investigated in preclinical studies and clinical trials. Developing effective therapies for this hard-to-treat cancer would be valuable.
Similarly, triple-negative breast cancer (TNBC) has been challenging researchers for years because it can’t be treated in the same manner as hormone-positive breast cancers. However, several studies have shown that CAR-T cells are potent at killing TNBC tumor cells.
An intercellular adhesion molecule 1 (ICAM 1)- specific CAR-T cell has also shown preclinical efficacy for treating advanced thyroid cancer. More research is needed in targeting solid cancers such as breast and thyroid tumors, but these preliminary results bode well for treating these diseases.
CAR-T trial results for autoimmune diseases, fibrosis, type 1 diabetes, and HIV
Targeting antigens with genetically engineered T cells can be applied to conditions other than cancer. Researchers are already beginning to unlock promising new treatments for diseases that have resisted effective ones so far. Autoimmune diseases are a specific area of interest.
Chimeric auto-antibody receptor (CAAR) T cells with the specificity of Dsg3 autoantigen were shown to kill autoimmune B cells without induction widespread immune suppression. Animal studies show that CAR-T cell therapy may be able to treat asthma — recent research used this method to target eosinophils that cause inflammation of the airways, which cured symptoms in mice. Targeting the antigen CD19 also revealed positive results in treating lupus, albeit in a small study.
Cardiac and liver fibrosis are currently being studied for CAR-T cell therapy after the discovery of a unique endogenous marker for cardiac fibroblasts. Researchers assessed the potency of CAR-T cells that target activated heart fibroblasts through the recognition of fibroblast activation protein (FAP) in mice with induced hypertensive cardiac injury and fibrosis. They found that anti-FAP CAR-T cells induced significant reductions or even eliminated cardiac fibrosis.
CAR-T cell therapy is also being used to treat type 1 diabetes. Fishman et al. created a multi-specific CAR-T cell with a receptor targeting different epitopes on the MHC 1 complexes of autoreactive CD8 T cells. Zhang et al. proposed another approach to treating diabetes with CAR-T cells in which a monoclonal antibody (mab287) that recognizes a common MHC-II/insulin peptide complex was engineered into a CAR-T cell.
Lastly, HIV may be a target for CAR-T cell therapy, signaling a potential breakthrough in treating this complex disease. CARs constructed based on neutralizing antibodies with a single chain as the binding domain have been applied to treat HIV, resulting in enhanced killing of both the virus and infected cells in vitro. The earliest trials of this type of therapy took place in the 1990s, but the use of new CAR sequences has shown better efficacy in these more recent research efforts.
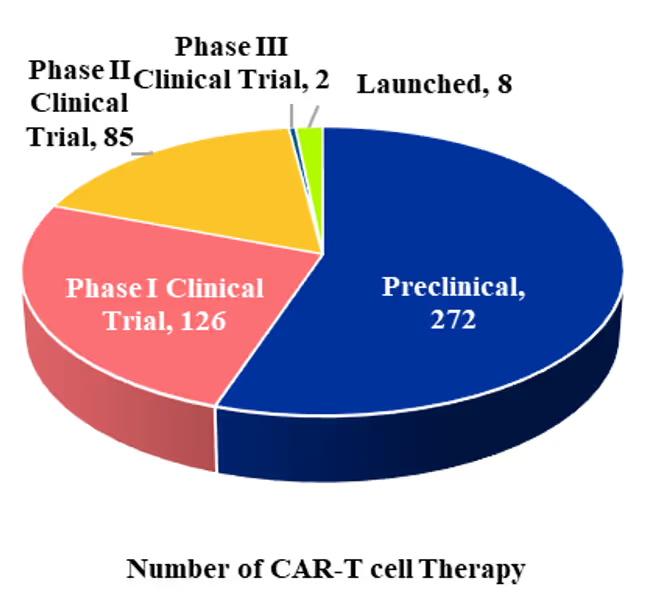
There are over 400 clinical trials in progress, although slightly more than half are in the preclinical stage (see Figure 5). This demonstrates the high potential for breakthroughs with this therapeutic approach, but underscores how much there still is to learn and refine.

Challenges facing CAR-T cell therapy
Controlling or reducing side effects will be crucial for bringing CAR-T cell therapy into wider clinical usage. CAR-T cell therapy causes cytokine release storms (CRS) in the body, resulting in a broad range of clinical symptoms such as fever, tachycardia and pyrexia, or even death. Neurotoxicity, usually associated with CRS, is also a risk as CAR-T cells migrate into the cerebrospinal fluid and release cytokines.
The on-target off-tumor effect is another issue to address. This occurs when a targeted antigen is expressed in healthy tissues and cancerous tumors. Researchers are now developing multi-specific CAR-T cells that recognize more than one antigen. Additional advancements known as Boolean logic gated CAR-T cells have recently been developed to promote the CAR-T cells’ specificity, control their activities, and overcome limitations associated with conventional CARs.
For example, inhibitory CARs (iCARs) are tailored to incorporate inhibitory signaling rather than activation domains as the internal signaling component of the off-target CAR construct. This makes it an important strategy to prevent the occurrence of on-target off-tumor toxicity.
Beyond specific side effects and efficacy, CAR-T cell therapy is challenging because of its personalized nature. Developing the requisite CARs is time-consuming and expensive, but if CAR-T cells could be created from donors rather than each individual patient, availability would increase and costs would decrease.
New manufacturing processes can help as well. For example, FasT CAR-T lowered the manufacturing time to just 24 hours, and this method showed promising efficacy for acute lymphoblastic leukemia. A recent study combined CRISPR-based genome editing technologies with virus-free gene-transfer strategies to generate CAR-T cells. These showed a similar phenotypic profile to non-edited CAR-T cells with equivalent in vitro and in vivo antitumoral efficacy.
These advances aren’t immediate answers to every challenge with CAR-T cell therapy, but they prove that it is possible to improve both the efficacy and economics of this treatment.
Opportunities to put the immune system on offense
CAR-T cell therapy has profoundly changed the treatment landscape of lymphoma, leukemia, and multiple myeloma, and these breakthroughs may next apply to solid tumors and even autoimmune conditions and diseases like type 1 diabetes and HIV that have resisted effective treatments. Innovations in manufacturing, such as automated processes and off-the-shelf CAR-T cells, will make treatments more accessible and cost-effective. With continued research and refinement of these therapies, CAR-T stands to use the body’s immune system as not just defense, but as an effective offensive force against diseases.




