
.avif)

Development and deployment of messenger RNA (mRNA) vaccines for SARS-CoV-2 was a tremendous public health achievement in the face of a global health crisis. That success generated immense excitement around mRNA technology, significantly accelerating its development and application to a wide range of diseases.
About 70% of active mRNA vaccine preclinical and clinical trials worldwide are now focused on diseases beyond COVID-19, comprising 31% of mRNA vaccine trials on cancer and 69% on other infectious, genetic, and immune diseases (see Figure 1). The surge of research into these vaccines since 2020 is surpassing COVID-19, proving they’ll be a long-term avenue for research and development.

The state of mRNA vaccine research
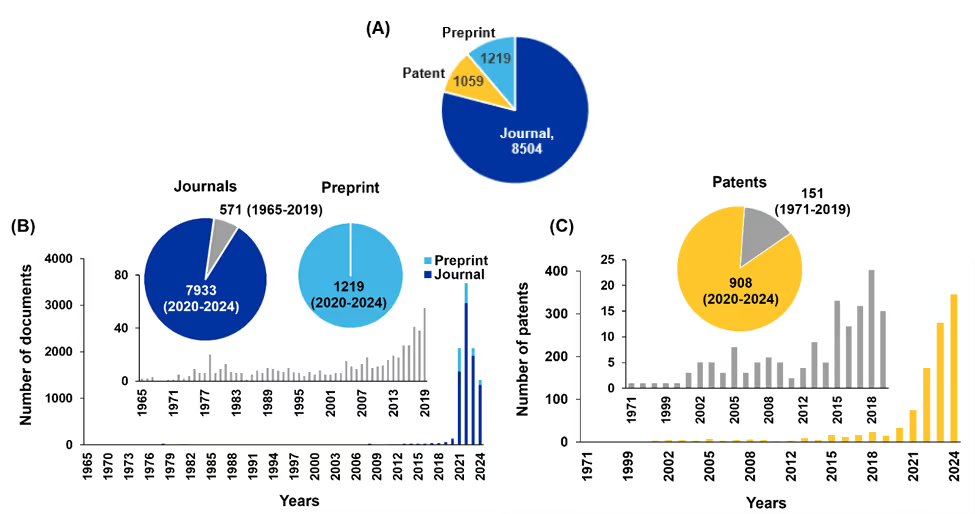
Although it may appear that mRNA vaccines were invented recently, research into these types of vaccines has been ongoing for over 30 years. As indicated in the CAS Content CollectionTM, the largest human-curated repository of scientific information, the output of journal publications in the mRNA vaccine field followed a slow upward trend from 1965 to 2019, with slight annual growth. The number of journal publications on mRNA vaccines was only 571 until 2019 (see Figure 2B).
Significant growth began in 2020, and by 2024, there were more than 8,000 journal publications relating to mRNA vaccines. Patents also reflect this trend, with mRNA vaccine patent publications increasing from around 30 in 2020 to several hundred in 2024 (see Figure 2C). The notable rise in preprint publications from 2020 to 2024 can be attributed to the urgent need to disseminate research findings on mRNA vaccines during the pandemic.
While COVID-19 understandably dominated the research landscape in the early years of this decade, the infrastructure and innovations established during the pandemic are now being applied to other diseases, including cancer, HIV, and rare diseases. As shown in Figure 1A, by December 2024, there were 280 vaccines in developmental stages, with 55% in the preclinical stage and 45% in various clinical stages.
COVID-19 was the catalyst for large-scale mRNA vaccine development, but this technology is now on a long-term path of research and development to address a range of challenging diseases.
What is mRNA?
mRNA is a single-stranded macromolecule comprised of nucleotide subunits, which can carry the genetic sequence of corresponding DNA and be read by ribosomes for the translation of protein in the cytoplasm. At the core of mRNA vaccine technology is the use of synthetic mRNA, designed to encode specific antigens (see Figure 3A).

Untranslated regions (UTRs), a 5’ cap, and a 3’ poly(A) tail flank the coding region and nucleosides within the mRNA are modified (Figure 3D) to delay degradation in the cytoplasm, decrease immunogenicity, and enhance translation. Once delivered into cells, these vaccines must be translated into antigens using the host cell’s translation machinery to trigger antigen-specific immune responses.
The translated antigens can be secreted and absorbed by cells as exogenous antigens, stimulating MHC class II-mediated immunity. Additionally, when mRNA vaccines are delivered to antigen-presenting cells (APCs), the translated antigens are perceived by the host as endogenous antigens, primarily activating MHC class I immune responses. The mRNA strand gets broken down by nucleases and has a short half-life.
This method is highly promising, but mRNA can be degraded by extracellular RNases, which may lead to failed translation and internalization by APCs. It can also struggle to cross the anionic cellular membrane. However, two key breakthroughs made mRNA vaccines possible: using lipid nanoparticles (LNPs) as mRNA delivery materials and chemically modifying mRNA to avoid unwanted immune responses.
LNPs for mRNA vaccine delivery are the only drug delivery system that has demonstrated clinical effectiveness and received approval for human use. In 2023, two scientists at the University of Pennsylvania, Dr. Katalin Karikó and Dr. Drew Weissman, won the Nobel Prize in Physiology or Medicine for their breakthroughs in chemically modifying mRNA bases that have significantly impacted mRNA stability, translation efficiency, and immune evasion.
Types of mRNA vaccines
There are three types of mRNA vaccines currently: non-replicating mRNA, self-amplifying RNA (saRNA), and circular RNA (circRNA).
- Conventional/non-replicating/non-amplifying mRNA: This type of mRNA vaccine consists of an ORF encoding for the proteins of interest, a 5’ cap structure, a 5’ UTR, a 3’ UTR, and a poly(A) tail that can be transcribed to one copy of immunogenic protein (Figure 3A). The immune response is directly proportional to the number of transcribed mRNAs. While these vaccines can be produced quickly and cost-effectively, they must be administered repeatedly because of the mRNA’s short half-life.
- Self-amplifying (saRNAs) and trans saRNAs: In addition to the conventional elements of linear mRNA, saRNA contains a long ORF sequence that encodes a viral replicase (nonstructural proteins; nsP1–nsP4), derived from alphaviruses, to amplify mRNA in the host cells (Figure 3 B). These vaccines are also easy to produce at scale and produce more antigens at lower doses than conventional mRNAs. However, synthesis can be difficult, and the large replicon size (~10 kb) limits cell internalization. saRNAs may be divided into a set of two taRNAs (Figure 3C), the mRNA without nsP1–nsP4 and the mRNA that encodes nsP1–nsP4 genes, to avoid large size and low encapsulation efficiency.
- Circular mRNAs (circRNAs): This type of mRNA vaccine contains a closed-loop structure with no 5’ and 3’ UTR. CircRNA is produced from mRNA precursors through back-splicing. The initiation of circRNA translation is independent of the 5’ cap structure. It translates proteins by rolling circle amplification (RCA). The closed-loop structure protects circRNAs from exonuclease degradation, and these vaccines with LNP carriers are highly stable. However, more safety testing is needed before being approved for clinical usage.
mRNA vaccines for conditions beyond COVID-19
The advancement of mRNA vaccines for infectious diseases beyond COVID-19 has shown consistent progress over the years (see Figure 4). Influenza represents half of the clinical trials in this area of study, followed by RSV, HIV, and the varicella zoster virus. Before 2020, research primarily focused on diseases like influenza, HIV, and HPV, with early clinical trials demonstrating the potential of mRNA technology. The success of mRNA COVID-19 vaccines in 2020 spurred expanded efforts targeting chlamydia, CMV, Epstein-Barr virus, hepatitis B, hepatitis C, malaria, inflammatory bowel disease, and Zika virus by 2021.

Multivalent vaccines for influenza (quadrivalent influenza mRNA vaccine MRT-5413, NCT05650554) and RSV progressed to late-stage trials in 2022, while early-phase studies began for diseases such as chikungunya, Nipah, HSV, rabies, yellow fever, varicella zoster, and multi-component vaccines (e.g., influenza and RSV; influenza, RSV, and SARS-CoV-2).
Emphasis centers on expanding mRNA vaccine platforms to tackle unmet needs in the future, including dengue, Ebola, heartland virus, gonorrhea, Japanese encephalitis, Lassa virus, Marburg virus, mpox, human metapneumovirus, phlebovirus, and tuberculosis, highlighting significant growth in this field. Moderna recently secured substantial funding from the U.S. government to develop mRNA-based vaccines for bird flu, aiming to prepare for potential human outbreaks.
Another exciting development is using mRNA vaccines to induce a robust T-cell response and eradicate cancer cells. In the 2010s, advancements in mRNA technology and delivery systems led to the initiation of early-phase clinical trials for personalized cancer vaccines targeting melanoma and other cancers. Efforts in mRNA vaccine research increased substantially after the successful deployment of COVID-19 vaccines.
More than 60 trials on mRNA cancer vaccines are currently listed for a range of cancers, including breast, ovarian, prostate, colon, metastatic renal cell, glioblastoma, melanoma, and solid tumors.Most are preclinical, but some have progressed to phase II (see Figure 5).

As pioneers in developing mRNA therapeutics, CureVac, Moderna, and BioNTech have designed a series of mRNA vaccines based on tumor-associated antigens (TAAs) and tumor-specific antigens (TSAs). Recently, Merck and Moderna initiated a phase III study (NCT05933577) evaluating V940 (mRNA-4157), which uses mRNA, encoding up to 34 neoantigens, in combination with KEYTRUDA® (pembrolizumab) for adjuvant treatment of patients with resected high-risk (stage IIB-IV) melanoma.
Recent advances in mRNA vaccine delivery
Choosing the right carrier is crucial for vaccine success and influences the immune response’s strength and precision. Advances in nanotechnology have enabled diverse carrier systems to improve mRNA delivery and expression in target cells. Table 1 presents the main delivery carriers focused on mRNA vaccine development, including LNPs, polymer-based nanostructures, and naturally-derived materials. These nanoparticle-based delivery systems protect administered mRNA from nuclease degradation, self-hydrolysis, and immune system threats. They also provide a versatile and targeted system for the safe delivery of mRNA to the target cells.
Table 1: Summary of nanoparticle-based platforms for mRNA delivery in mRNA vaccine technology. Adapted from Meng-Zhen Yu et al 2023. The clinical progress and challenges of mRNA vaccines - PubMed
Current limitations of mRNA vaccines and how to overcome them
Recent breakthroughs in mRNA vaccines prove that this is an effective technology that could be leveraged against many other diseases. However, challenges remain for future development, including issues related to the immunogenicity and stability of mRNA, biosafety concerns, targeting problems in delivery systems, and quality control for large-scale production of mRNA vaccines.
For example, coronaviruses like SARS-CoV-2 and influenza continually present new variants and strains, which require new vaccines. Therefore, researchers are working on multivariant boosters and universal vaccines for these types of viruses. The HIV virus also exhibits rapid mutations and proteoglycan-shielding that conceals critical epitopes. An mRNA vaccine would need to produce broadly neutralizing antibodies to be effective against HIV. Any mRNA vaccine would need to be thermostable to tackle a disease like Ebola. The only current FDA-approved vaccine for Ebola requires -80℃ storage, and there are no other mRNA Ebola vaccines in clinical development currently. Rabies, RSV, and malaria are also targets for potential mRNA vaccines, but each needs to demonstrate success in clinical trials.
Despite these challenges, the future of this technology is extremely promising. Decades of advancements in mRNA design and nucleic acid delivery technology, along with the identification of novel antigen targets, have positioned mRNA vaccines at the forefront of disease prevention and treatment. While a dramatic increase in mRNA research related to COVID-19 vaccines emerged, we see that other non-COVID-19 research and development technology now dominates preclinical and clinical trials, especially for infectious diseases and cancers. As research progresses, we can anticipate more innovative applications of mRNA technology.




